Conditions Evaluated
Spine-Related Pain
Evaluation.
The spine is a complex structure, and pain originating from or near it can have several possible sources. Dr. Dardashti evaluates spine-related pain through a careful history, physical and neurologic examination, and review of available imaging — to identify the most likely contributing structures.
In Brief
Multiple Possible Sources
Spine pain can arise from intervertebral discs, facet joints, the sacroiliac joint, nerve roots, or surrounding soft tissues. Identifying the likely contributor is central to evaluation.
Region Matters
Spine-related pain may be cervical (neck), thoracic (mid-back), or lumbar (low back) in origin. Each region has distinct anatomy and clinical features that guide evaluation.
Individualized Approach
Treatment is based on the specific pain source, severity, duration, prior treatment history, and the patient's functional goals — not a single imaging finding or symptom in isolation.
Overview
What Is Spine-Related Pain?
Spine-related pain broadly refers to pain that originates from or is closely associated with the structures of the vertebral column — including the cervical, thoracic, and lumbar regions. It is among the most common reasons patients are referred for pain medicine evaluation.
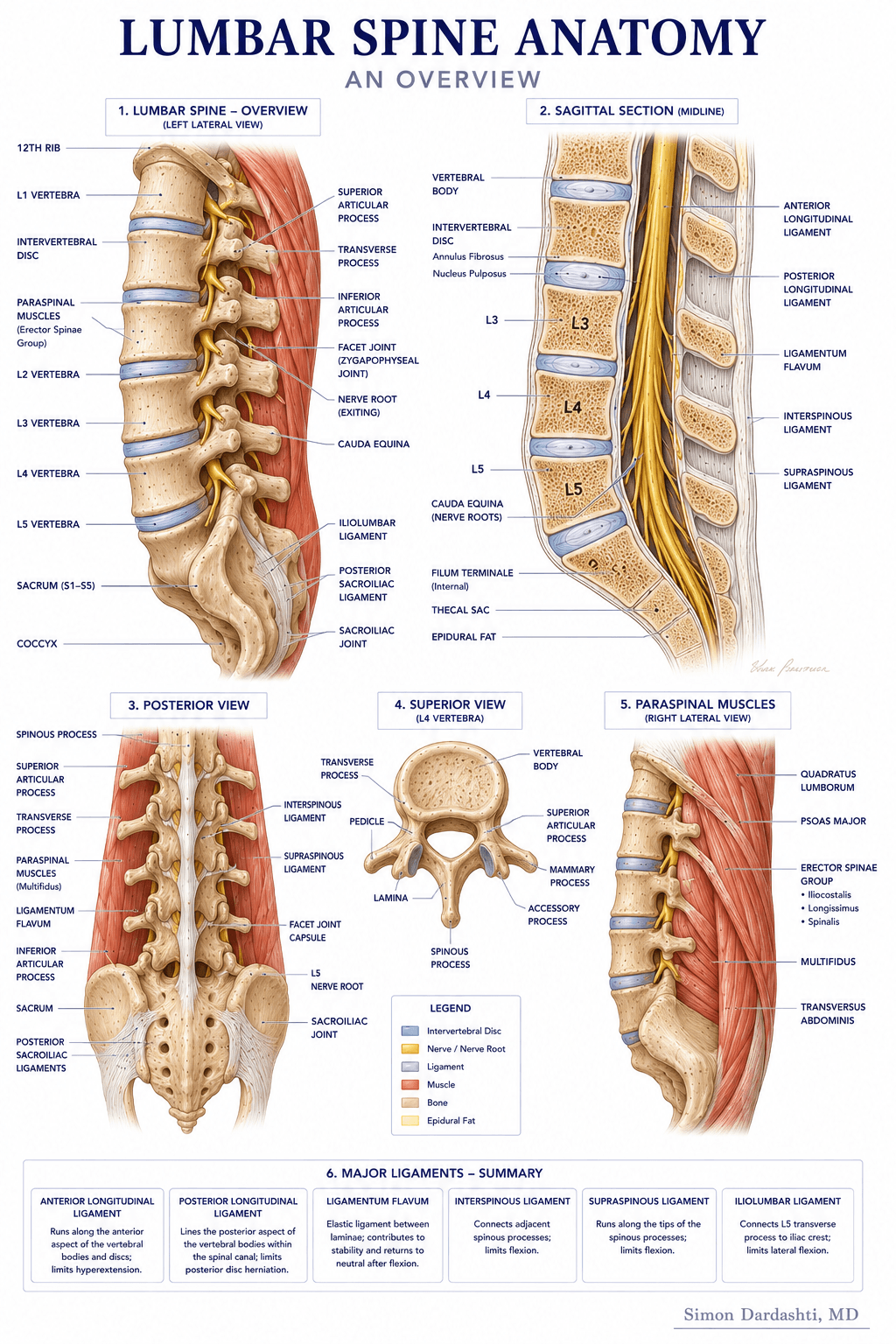
The spine contains many structures that can become sources of pain: intervertebral discs, facet joints, the sacroiliac joints, spinal nerve roots, ligaments, and paraspinal muscles. In some patients, more than one structure may be contributing, making accurate clinical evaluation important before treatment is planned.
Spine-related pain may be primarily axial — meaning localized to the neck, mid-back, or low back — or it may radiate into the arms or legs when nerve roots are involved. The character, distribution, and pattern of pain help guide the evaluation.
Sources
Common Sources of Spine Pain.
Spine-related pain may arise from one or more of the following structures:
- Intervertebral discs — including disc herniation, annular tears, or degenerative disc changes
- Facet joints — small paired joints at each spinal level that can become a source of axial pain
- Sacroiliac joints — the joints connecting the sacrum and the pelvis, which may contribute to low back and buttock pain
- Spinal nerve roots — which may be irritated or compressed, producing radicular or radiating symptoms
- Paraspinal muscles and ligaments — which can contribute to local pain, particularly following injury or prolonged mechanical stress
- Spinal stenosis — narrowing of the spinal canal or nerve exit foramina that may affect nerve roots or the spinal cord
Approach
How Dr. Dardashti Evaluates Spine-Related Pain.
Evaluation begins with a thorough history of the pain — including its location, character, onset, and pattern — along with relevant medical history, prior imaging, and prior treatments and their outcomes. Understanding which activities aggravate or relieve symptoms helps narrow the likely pain generator.
A physical and neurologic examination assesses posture, range of motion, palpation findings, and neurologic function. For patients with arm or leg symptoms, a neurologic exam helps determine whether nerve root involvement is likely and at which level.
When imaging is available — such as MRI, CT, or plain radiographs — findings are reviewed alongside the clinical picture. Imaging alone is not sufficient to determine the appropriate treatment; it must be interpreted in the context of the patient's symptoms and examination.
Treatment
Treatment Options That May Be Considered.
Treatment is individualized based on the suspected pain source and the full clinical evaluation. Options that may be considered include:
- Physical therapy coordination and activity modification guidance
- Medication management when clinically appropriate
- Epidural steroid injections for radicular or nerve-related symptoms
- Facet joint injections or medial branch blocks when facet-mediated pain is suspected
- Sacroiliac joint injections when sacroiliac joint involvement is a likely contributor
- Radiofrequency ablation for selected patients who respond to diagnostic nerve blocks
- Spinal cord stimulation evaluation for appropriate candidates with chronic refractory pain
Not every patient requires an interventional procedure. Recommendations are based on individual clinical evaluation, prior treatment history, and functional goals.
Limitations
Important Limitations.
Spine-related pain is often multifactorial, and the same imaging finding may be associated with different clinical presentations in different patients. No evaluation or treatment can be guaranteed to identify or resolve the pain source in every case.
A formal clinical evaluation is required to determine the appropriate diagnostic and treatment approach for any individual patient. This page is for general informational purposes only and does not constitute medical advice.
Dr. Dardashti sees patients in Mission Hills, California, serving patients from the San Fernando Valley, Santa Clarita Valley, and surrounding Los Angeles communities.
Medically Reviewed by Simon Dardashti, MD, MS·Board-Certified, Pain Medicine & Anesthesiology
Last Reviewed: July 2026