Conditions Evaluated
Facet-Mediated Pain
Evaluation.
Facet joints are small joints present at every level of the spine. When they become a primary source of pain, the condition is referred to as facet-mediated or facet joint pain. Dr. Dardashti evaluates this condition in the cervical, thoracic, and lumbar spine.
In Brief
Facet Joints as Pain Generators
Facet joints are paired joints at each spinal level that can become a significant source of axial neck, mid-back, or low back pain when they degenerate or become irritated.
No Single Defining Feature
Facet-mediated pain does not always show clearly on imaging. Clinical history, examination, and response to diagnostic nerve blocks are important parts of evaluation.
Targeted Diagnostic Options
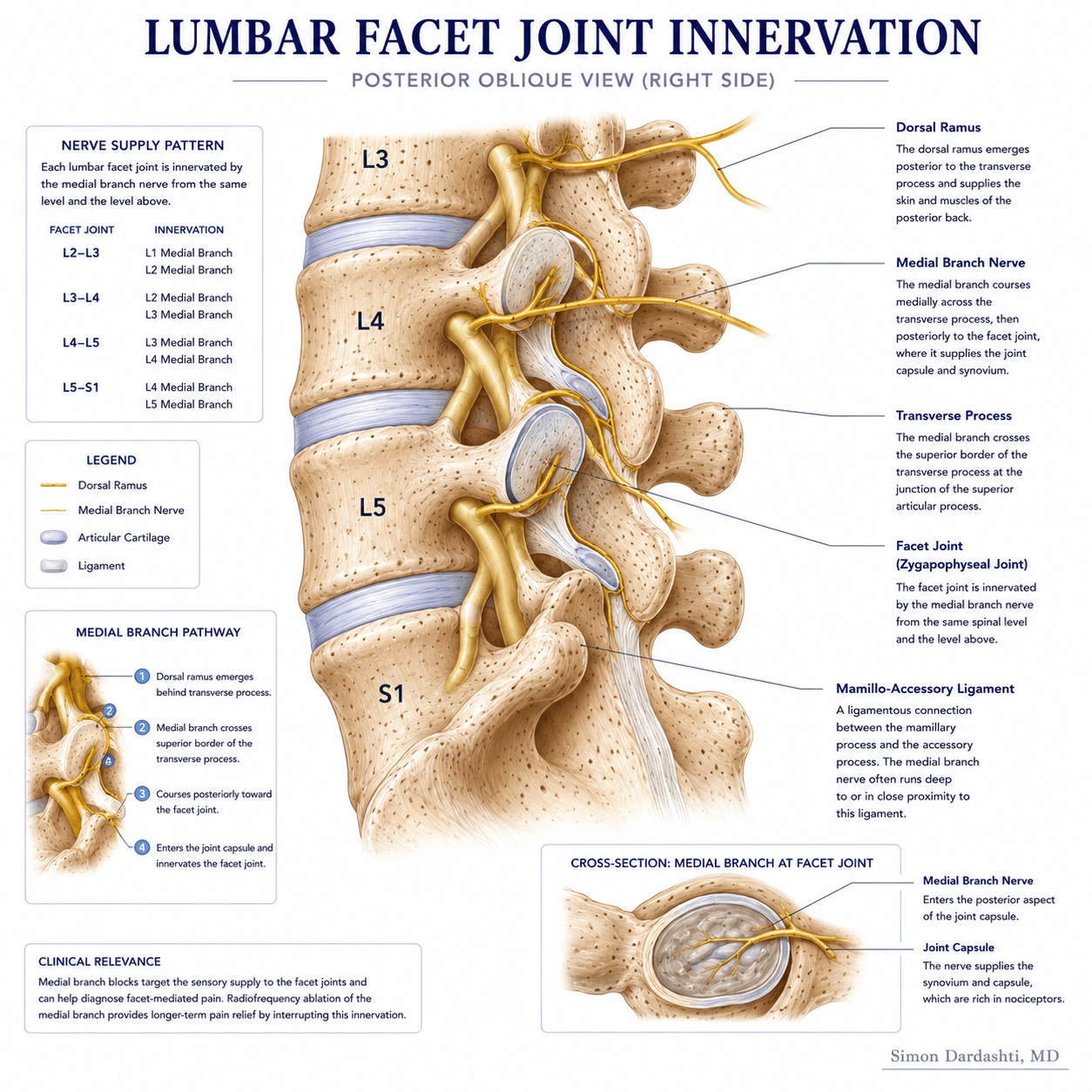
Medial branch blocks can be used to assess whether facet joints are contributing to pain. For confirmed cases, radiofrequency ablation may be considered in selected patients.
Overview
What Is Facet-Mediated Pain?
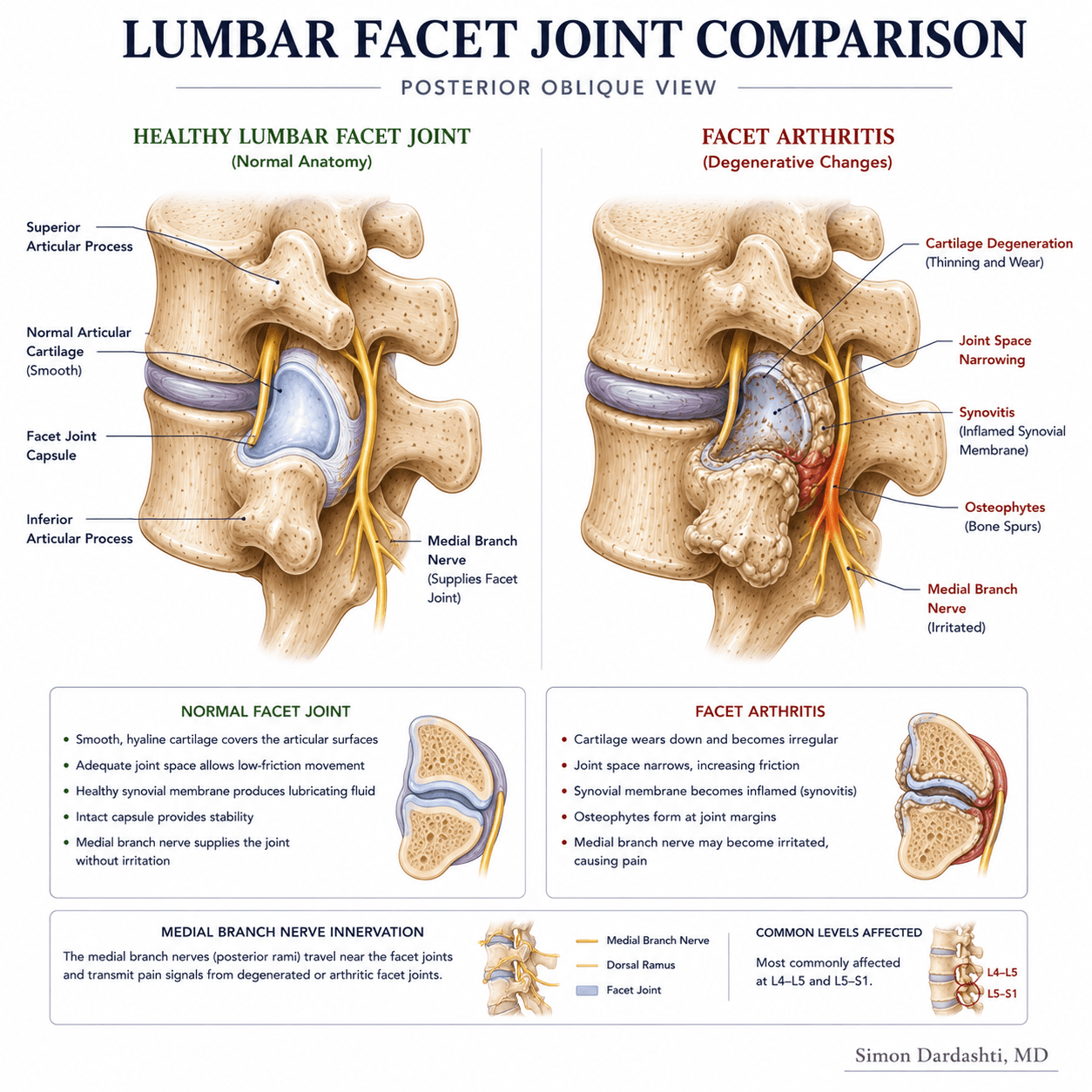
Facet joints — also called zygapophyseal joints — are paired synovial joints located at every vertebral level of the spine. They provide stability and guide movement between adjacent vertebrae. Like any joint in the body, facet joints can become arthritic, inflamed, or otherwise painful over time.
Facet-mediated pain refers to pain that is primarily generated by one or more facet joints. It is a recognized cause of axial neck pain, mid-back pain, and low back pain. The pain is typically described as a deep, aching discomfort that may refer to adjacent areas — for example, cervical facet pain may refer to the shoulder or head, while lumbar facet pain may refer to the buttock or upper thigh.
Unlike radicular pain, facet-mediated pain does not typically follow a specific nerve root pattern and usually does not cause neurologic symptoms such as numbness or weakness. However, the two conditions can coexist in the same patient.

Symptoms
Common Symptoms Associated With Facet Pain.
Symptoms that may suggest a facet joint contribution include:
- Axial neck, mid-back, or low back pain that is worse with extension or rotation
- Pain that is typically worse in the morning or after prolonged sitting
- Referred pain to the shoulder, buttock, or upper thigh without a specific nerve root pattern
- Tenderness on palpation near the facet joints
- Pain that improves with rest or forward flexion
- Absence of neurologic symptoms such as arm or leg weakness or numbness
These features are not diagnostic on their own. An accurate clinical evaluation is required to determine whether facet joints are the likely pain source.
Approach
How Dr. Dardashti Evaluates Facet-Mediated Pain.
Evaluation begins with a detailed history of pain location, character, onset, and aggravating and relieving factors. Physical examination assesses paraspinal tenderness, range of motion, and pain pattern.
Imaging — such as MRI or CT — may show degenerative changes at the facet joints, but these findings alone do not confirm that the facets are the source of pain. The correlation between imaging and clinical symptoms is imperfect, which is why diagnostic nerve blocks can play an important role in the evaluation process.
Medial branch blocks — image-guided injections that temporarily anesthetize the nerves supplying the facet joints — can provide useful diagnostic information. A positive response to a medial branch block suggests that facet joints are a likely contributor and may support consideration of radiofrequency ablation in appropriate patients.
Treatment
Treatment Options That May Be Considered.
Treatment is based on the clinical evaluation and the patient's prior treatment history. Options that may be considered include:
- Physical therapy and activity-based approaches to reduce facet joint loading
- Medication management when clinically appropriate
- Facet joint injections for diagnostic and potentially therapeutic purposes
- Medial branch blocks as a diagnostic step to assess facet contribution
- Radiofrequency ablation for selected patients with confirmed facet-mediated pain who respond to diagnostic blocks
- Reassessment and ongoing monitoring of treatment response
Not every patient with suspected facet-mediated pain requires an injection or ablation procedure. Recommendations are individualized based on clinical evaluation and goals.
Limitations
Important Limitations.
Facet-mediated pain cannot be diagnosed based on imaging alone, and no single clinical feature reliably confirms the diagnosis. Response to treatment varies among patients. Radiofrequency ablation does not provide permanent relief in all patients, and effects may diminish over time.
A formal clinical evaluation is required to determine whether facet-focused treatment is appropriate for any individual patient. This page is for general informational purposes only and does not constitute medical advice.
Dr. Dardashti sees patients in Mission Hills, California, serving patients from the San Fernando Valley, Santa Clarita Valley, and surrounding Los Angeles communities.
Medically Reviewed by Simon Dardashti, MD, MS·Board-Certified, Pain Medicine & Anesthesiology
Last Reviewed: July 2026