Conditions Evaluated
Myofascial Pain
Evaluation.
Myofascial pain refers to pain that originates from muscles and the surrounding connective tissue. It is a recognized source of regional pain that can occur on its own or alongside other conditions affecting the spine, joints, or nervous system. Dr. Dardashti evaluates myofascial pain as part of a comprehensive assessment of the patient's overall pain picture.
In Brief
Muscle and Soft-Tissue Pain
Myofascial pain arises from muscles and their surrounding fascia. It is often characterized by localized tenderness and reproducible referred pain patterns that can be provoked by pressure on specific points within muscle tissue.
Overlapping With Other Conditions
Myofascial pain frequently coexists with spine pain, joint pain, or radicular symptoms. It is often underrecognized as a contributing factor in patients with complex or persistent pain.
Multimodal Approach
Management of myofascial pain typically emphasizes physical approaches, activity modification, and posture-related factors. Treatment is individualized and takes into account any overlapping pain conditions.
Overview
What Is Myofascial Pain?
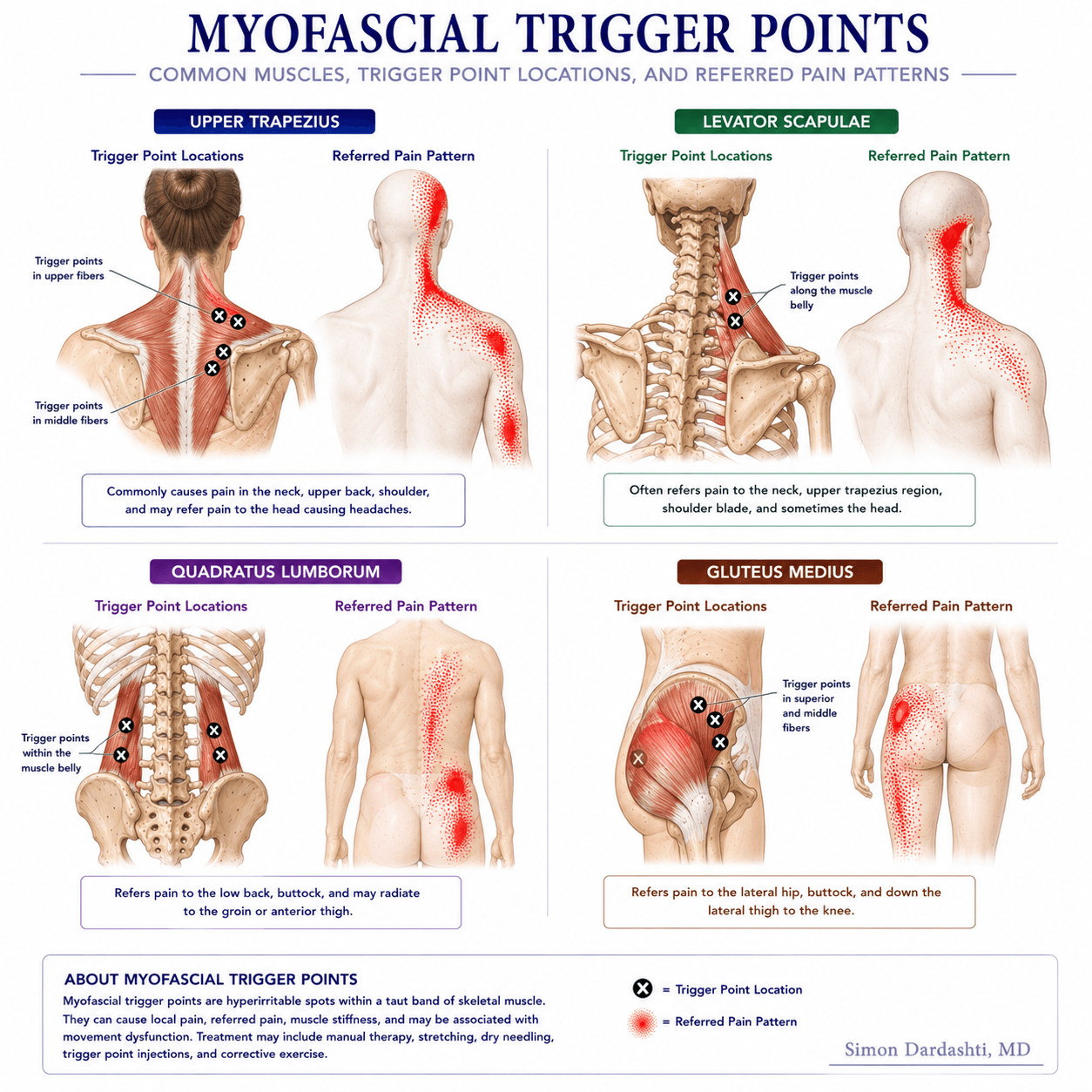
Myofascial pain syndrome is a regional pain condition characterized by the presence of trigger points — localized areas within a muscle or its fascia that are tender to palpation and may produce a characteristic pattern of referred pain when compressed. The referred pain from a trigger point may be felt at a distance from the trigger point itself, which can sometimes make the source of pain difficult to identify.
Myofascial pain can develop following injury, repetitive strain, sustained postures, or periods of physical or emotional stress. Affected muscles vary by patient and clinical context, but the paraspinal muscles, trapezius, gluteal muscles, and hip flexors are among those commonly involved in patients with spine and musculoskeletal pain complaints.
The condition can exist in isolation or alongside other pain sources such as disc degeneration, facet joint pain, or joint pathology. In some patients, it is a significant contributor to the overall pain burden even when other structural findings are present on imaging.
Presentation
Common Features and Presentations.
Myofascial pain may present in a variety of ways. Common features include:
- Regional aching or tightness in a muscle group, often aggravated by sustained posture or overuse
- Reproducible tenderness at specific points within the muscle
- Referred pain felt at a location distant from the tender spot
- Pain that is worsened by prolonged sitting, standing, or repetitive activity
- Stiffness or reduced range of motion in the affected region
- Symptoms that may fluctuate with stress, fatigue, sleep quality, or activity level
Approach
How Dr. Dardashti Evaluates Myofascial Pain.
Evaluation includes a thorough history of pain onset, location, character, and aggravating factors — including occupational and activity-related patterns. The relationship of symptoms to posture, sleep, and prior treatments is also assessed.
Physical examination includes palpation of the muscles in the affected region to identify tenderness, trigger points, and referred pain patterns. This is performed alongside assessment of range of motion and an evaluation of any underlying structural contributors — including the spine and adjacent joints.
Myofascial pain can accompany or be secondary to other pain sources. When both myofascial and structural contributors are present, the evaluation considers the relative contribution of each to guide treatment prioritization.
Treatment
Treatment Options That May Be Considered.
Treatment of myofascial pain is typically multimodal and individualized based on the severity, contributing factors, and prior treatment history. Options that may be considered include:
- Physical therapy with a focus on stretching, posture correction, and soft-tissue techniques
- Activity modification and ergonomic guidance when occupational or postural factors contribute
- Medication management when clinically appropriate
- Trigger point injections for selected patients when discrete, reproducible trigger points are identified
- Addressing co-existing structural pain sources — such as facet joints or the sacroiliac joint — that may perpetuate muscle guarding
- Multimodal pain management planning when myofascial pain is part of a broader chronic pain presentation
Treatment recommendations are individualized. Not every patient requires injections, and addressing contributing postural or structural factors is often a central part of management.
Limitations
Important Limitations.
Myofascial pain is a clinical diagnosis based on history and physical examination. It does not typically show on standard imaging. The extent to which it contributes to a patient's overall pain can be difficult to quantify, and treatment response varies among patients.
A formal clinical evaluation is required to determine the appropriate treatment approach. This page is for general informational purposes only and does not constitute medical advice or create a physician-patient relationship.
Dr. Dardashti sees patients in Mission Hills, California, serving patients from the San Fernando Valley, Santa Clarita Valley, and surrounding Los Angeles communities.
Related
Medically Reviewed by Simon Dardashti, MD, MS·Board-Certified, Pain Medicine & Anesthesiology
Last Reviewed: July 2026