Procedures & Treatment Options
Kyphoplasty
for Compression Fractures.
Kyphoplasty is a minimally invasive, image-guided procedure used for selected patients with painful vertebral compression fractures. It may be considered when pain is significant, limiting function, and conservative care has been insufficient.
In Brief
Painful Compression Fractures
Kyphoplasty is a minimally invasive, image-guided procedure for selected patients with painful vertebral compression fractures that limit function and mobility.
Fracture Stabilization
The procedure aims to stabilize the fractured vertebra and, in some cases, partially restore vertebral body height under careful clinical guidance.
Careful Patient Selection
Kyphoplasty is not appropriate for every fracture. Thorough evaluation of imaging, symptoms, and clinical context is essential before considering the procedure.
Overview
What Is a Vertebral Compression Fracture?
Kyphoplasty is a minimally invasive, image-guided procedure used in selected patients with painful vertebral compression fractures. These fractures can occur when a vertebral body weakens and partially collapses. Common causes include osteoporosis, trauma in weakened bone, and in some cases tumor-related or pathologic fractures.
The goal is to stabilize the painful fractured vertebra and, in some cases, partially restore vertebral body height. A careful evaluation is needed to determine whether the fracture is likely the source of pain and whether kyphoplasty is appropriate.
A vertebral compression fracture occurs when one of the bones of the spine collapses or loses height. This can cause sudden back pain, pain with standing or walking, difficulty with movement, and reduced function. Compression fractures are often associated with osteoporosis, but not all compression fractures require a procedure.
Candidacy
When Kyphoplasty May Be Considered.
Kyphoplasty may be considered when:
- A vertebral compression fracture appears to be a likely source of significant pain
- Pain is limiting function, mobility, standing, walking, or basic daily activities
- Imaging supports an acute or subacute fracture at a level that matches the patient's symptoms
- Conservative care has not provided adequate relief, or pain severity makes prolonged immobility risky
- The fracture pattern appears anatomically appropriate for the procedure
Dr. Dardashti reviews your clinical history, imaging, and overall health to determine whether kyphoplasty may be appropriate.
Limitations
When Kyphoplasty May Not Be Appropriate.
Kyphoplasty is not appropriate for every patient or every fracture. It may not be appropriate when pain is improving with conservative care, the fracture is old and no longer active, there is significant neurologic compromise, unstable burst fracture pattern, spinal infection, sepsis, uncorrected bleeding risk, or other anatomic concerns.
Dr. Dardashti reviews the clinical history, neurologic symptoms, imaging, medications, and overall medical situation before considering whether kyphoplasty is reasonable.
Procedure
How the Procedure Is Performed.
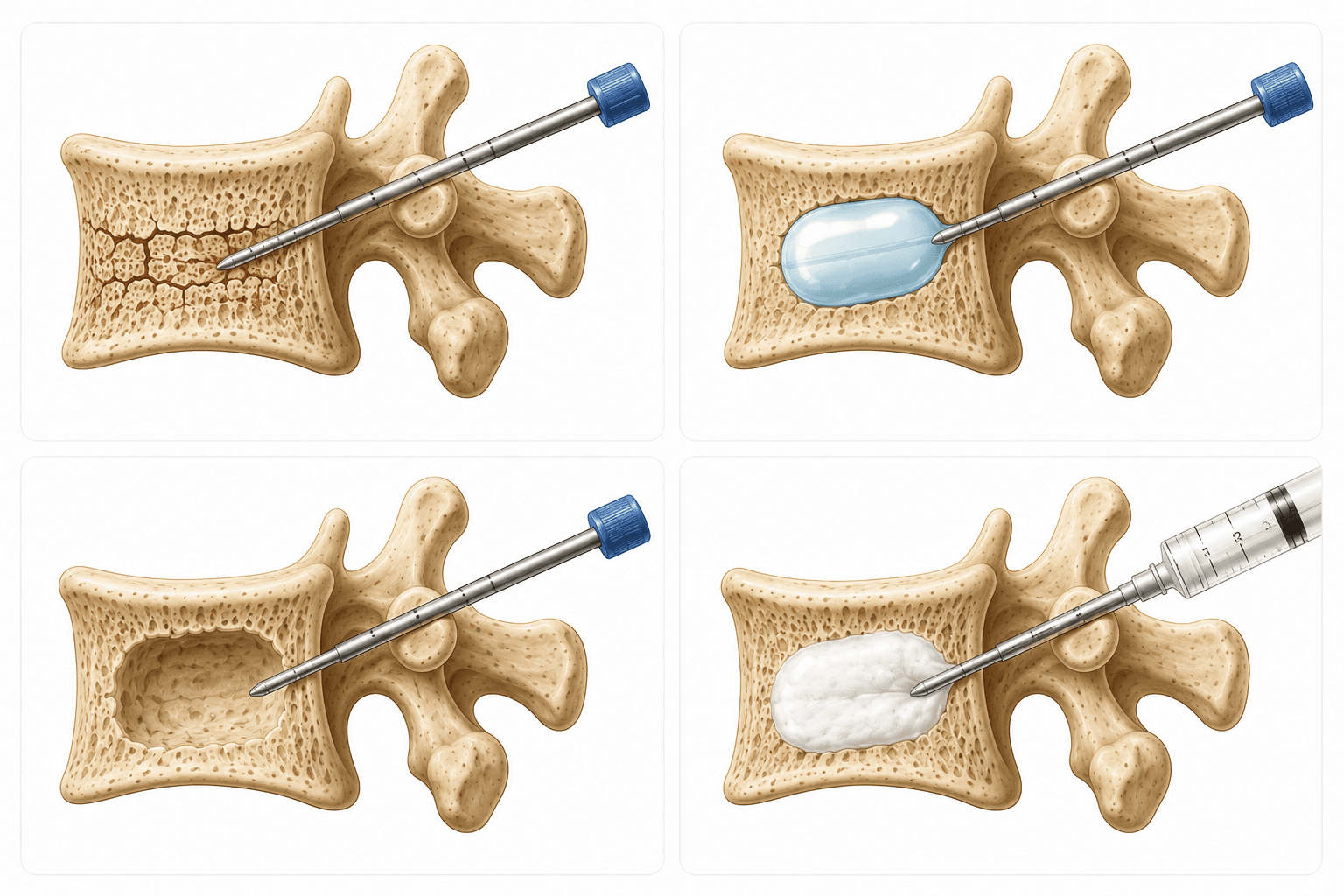
The procedure is performed using image guidance, usually fluoroscopy. The patient lies face down. The skin is cleaned and numbed. A small needle or cannula is guided into the fractured vertebra. A small balloon may be used to create a cavity and help restore some vertebral height. Medical bone cement is then placed into the vertebra to stabilize the fracture.
During the procedure, you may feel pressure or mild sensations. After the procedure, temporary soreness at the site is common. The duration of the procedure and recovery depends on individual factors and the specific clinical situation.
Recovery
What to Expect Afterward.
Some patients notice improvement quickly, while others have more gradual or incomplete improvement. Temporary soreness at the procedure site can occur. Activity instructions depend on the patient's fracture, bone health, sedation, other medical conditions, and the treating physician's recommendations.
Pain improvement varies widely. There is no guarantee of immediate or complete pain relief. Your physician will discuss what to expect and provide guidance on activity, medications, and follow-up care.
Risks
Risks and Considerations.
Risks are uncommon but may include temporary soreness, bleeding, infection, cement leakage, nerve irritation or neurologic injury, allergic reaction, worsening pain, failure to improve, or need for additional treatment. Patients with osteoporosis may also remain at risk for future fractures.
All potential risks and how they apply to your specific situation should be discussed in detail with Dr. Dardashti before any procedure is performed.
Treatment Plan
How This Fits Into a Broader Treatment Plan.
Kyphoplasty addresses pain from a selected painful vertebral compression fracture. It does not treat the underlying cause of bone weakness. A broader plan may include osteoporosis evaluation and treatment, fall-risk reduction, physical therapy or rehabilitation, medication review, and coordination with the patient's primary care physician, endocrinologist, oncologist, or spine specialist when appropriate.
Dr. Dardashti works with your overall medical team to ensure that any intervention is part of a comprehensive, coordinated treatment approach.
FAQ
Frequently Asked Questions.
What is kyphoplasty?
Kyphoplasty is a minimally invasive, image-guided procedure used for selected patients with painful vertebral compression fractures. Using fluoroscopy for guidance, the procedure involves stabilizing the fractured vertebra and sometimes partially restoring vertebral body height using medical-grade bone cement.
What type of fracture does kyphoplasty treat?
Kyphoplasty may be used for vertebral compression fractures — fractures where a vertebral body loses height due to osteoporosis, trauma, tumor-related changes, or other causes. Not all compression fractures require kyphoplasty, and careful evaluation is needed to determine if the fracture is contributing to a patient's pain.
Is kyphoplasty the same as vertebroplasty?
Kyphoplasty and vertebroplasty are related but distinct procedures. Kyphoplasty uses a balloon to create space and potentially restore some vertebral height before cement placement. Vertebroplasty typically places cement directly into the fractured vertebra without the balloon step. Dr. Dardashti discusses which approach, if either, may be appropriate for each patient.
How do you know if a compression fracture is causing my pain?
Determining whether a compression fracture is responsible for pain requires a complete clinical evaluation: review of your pain pattern, examination findings, imaging characteristics, the age of the fracture, and how symptoms correlate with the fracture location. A single imaging finding does not define the diagnosis — the full clinical picture matters.
Does kyphoplasty treat osteoporosis?
No. Kyphoplasty addresses pain from a selected painful compression fracture. It does not treat the underlying bone weakness or osteoporosis. A broader treatment plan often includes osteoporosis evaluation, appropriate medical management, fall prevention, and coordination with your primary care physician, endocrinologist, or bone specialist.
How soon might pain improve after kyphoplasty?
Pain improvement varies among patients. Some patients notice improvement within days or weeks; others experience more gradual improvement. Some patients experience partial or incomplete improvement. There is no guarantee of immediate or complete pain relief, and recovery depends on the fracture, bone quality, overall health, and other factors.
What are the risks of kyphoplasty?
Risks, while uncommon, may include temporary soreness or discomfort at the procedure site, bleeding, infection, cement leakage into surrounding tissues, nerve irritation or neurologic injury, allergic reaction, worsening pain, or failure to improve. Patients with osteoporosis also remain at risk for future fractures. All risks should be discussed with Dr. Dardashti before any procedure.
Are all compression fractures treated with kyphoplasty?
No. Kyphoplasty is not appropriate for all compression fractures. Many compression fractures improve with conservative care, activity modification, and time. Kyphoplasty is considered only when pain is significant, limiting function, conservative care has been insufficient, and imaging and clinical findings support the fracture as a likely pain source.
Important Information
Important Limitations.
This content is for general informational purposes only and does not constitute medical advice, a diagnosis, or a guarantee of specific treatment outcomes. Every patient's situation is unique, and treatment recommendations are individualized based on clinical evaluation.
Kyphoplasty is not appropriate for all patients or all compression fractures. Not all patients experience pain relief or improvement after kyphoplasty. Response varies, and some patients may experience partial benefit or no improvement.
Dr. Dardashti sees patients in Mission Hills, California, serving patients from the San Fernando Valley, Santa Clarita Valley, and surrounding Los Angeles communities. A formal clinical evaluation is required to determine whether any treatment is appropriate.
Medically Reviewed by Simon Dardashti, MD, MS·Board-Certified, Pain Medicine & Anesthesiology
Last Reviewed: July 2026