Conditions Evaluated
Occipital Neuralgia
Evaluation.
Occipital neuralgia is characterized by sharp, shooting pain in the back of the head and scalp, resulting from irritation of the occipital nerves. Dr. Dardashti evaluates occipital neuralgia in the context of symptom character, physical examination findings, and response to diagnostic interventions.
In Brief
Occipital Nerve Involvement
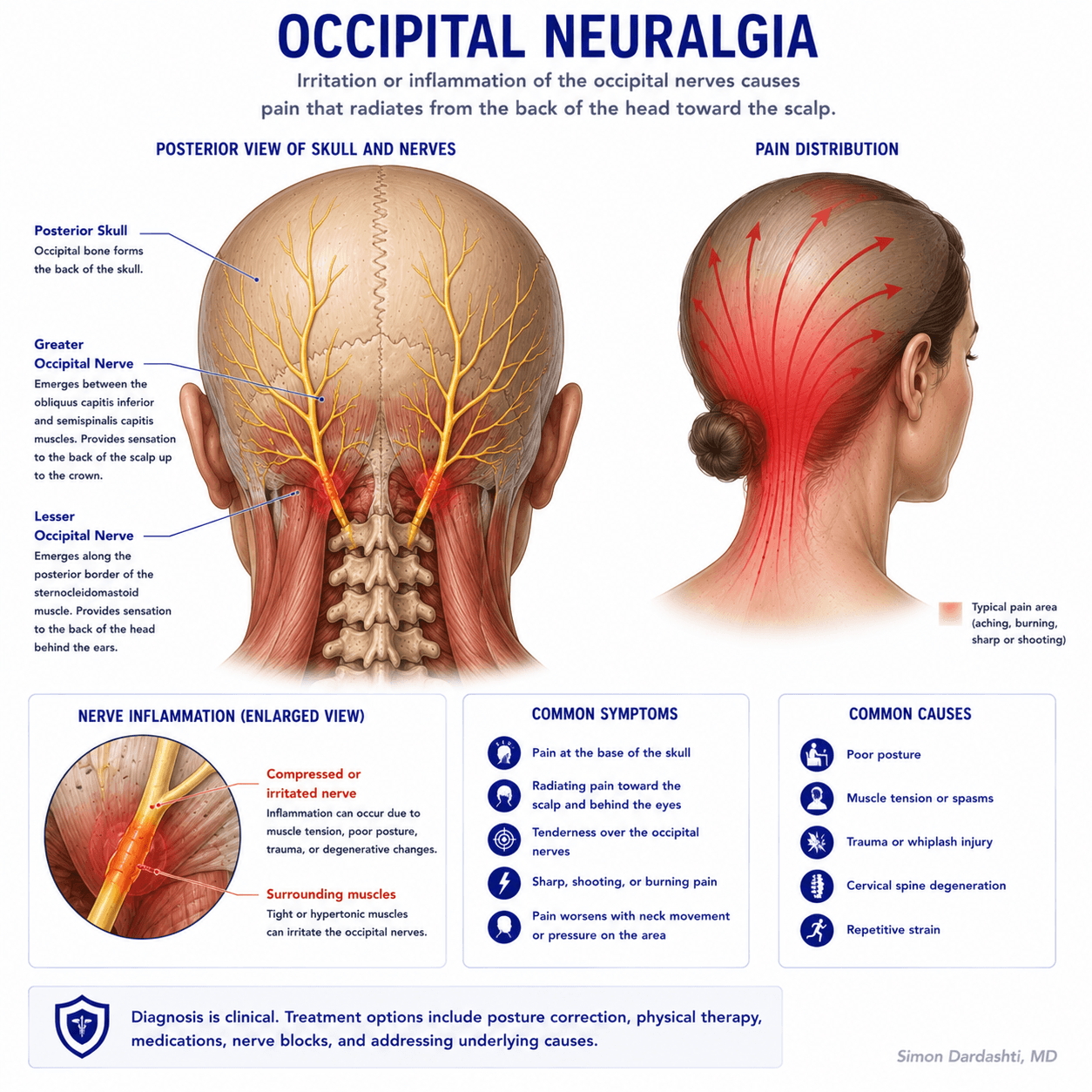
Occipital neuralgia results from irritation or compression of the greater or lesser occipital nerves, which supply sensation to the back of the head and scalp.
Sharp, Electric Pain
Characteristic symptoms include sharp, shooting, or electric pain in the back of the head, often with scalp tenderness and sensitivity. Pain may be one-sided or bilateral.
Distinct from Migraine
Occipital neuralgia differs from migraines and tension headaches. Accurate diagnosis requires careful clinical evaluation of symptom character, location, and associated features.
Overview
What Is Occipital Neuralgia?
Occipital neuralgia is a condition characterized by sharp, shooting, or electric pain in the distribution of the occipital nerves, which supply sensation to the back of the head and scalp. The pain typically originates at the base of the skull and radiates upward toward the crown or side of the head. Symptoms may be unilateral (one-sided) or bilateral (affecting both sides).
The greater and lesser occipital nerves originate from the upper cervical spine (specifically from nerve roots C2 and C3). These nerves travel upward through the neck muscles and fascia to supply sensation to the scalp. When these nerves are irritated or compressed, occipital neuralgia can develop.
Occipital neuralgia is distinct from migraines and tension headaches, though pain in the occipital region can sometimes accompany other headache types. Accurate diagnosis requires careful evaluation of the characteristic symptoms and pain pattern.
Symptoms
Symptoms of Occipital Neuralgia.
Typical symptoms include:
- Sharp, shooting, or electric pain in the back of the head
- Pain that radiates from the base of the skull upward toward the crown
- One-sided or bilateral pain depending on nerve involvement
- Scalp tenderness or sensitivity to touch, combing, or pressure
- Pain that may worsen with neck movement or certain positions
- Intermittent or continuous pain that varies in intensity
- Possible numbness or altered sensation in affected areas
Symptoms may be constant or episodic and vary significantly among patients. Some individuals experience brief, intense bursts of pain, while others report more persistent discomfort.
Causes
Common Causes and Contributing Factors.
Occipital neuralgia can result from compression or irritation of the occipital nerves at various points along their course. Common causes and contributing factors include:
- Tension in the neck and suboccipital muscles
- Cervical spine pathology, such as disc herniation or arthritis
- Trauma or whiplash injury to the neck
- Repetitive neck strain from poor posture or prolonged computer use
- Tight neck muscles that compress the nerve pathway
- Compression from surrounding anatomical structures
- Prior neck injury or surgery
In many cases, no clear precipitating event or identifiable cause is found, and occipital neuralgia is diagnosed based on characteristic symptoms and clinical findings.
Diagnosis
How Occipital Neuralgia Is Diagnosed.
Diagnosis begins with a detailed history of the pain — its character, location, duration, and pattern — along with any aggravating or relieving factors. The physical examination includes palpation along the course of the occipital nerves to identify tender points and attempts to reproduce symptoms through specific maneuvers.
Neurologic examination may assess sensation and motor function in the affected area. Imaging such as cervical MRI or CT may be ordered if there is clinical concern for cervical spine pathology or other structural issues.
Occipital nerve blocks serve both diagnostic and therapeutic purposes. When an occipital nerve block with local anesthetic provides meaningful relief, this finding supports the diagnosis of occipital neuralgia and can guide further management decisions.
Treatment
Treatment Options That May Be Considered.
Treatment is individualized based on symptom severity, duration, and response to initial approaches:
- Physical therapy, including neck stretches and postural correction to address muscular tension
- Medications such as neuropathic pain agents, muscle relaxants, or anti-inflammatory medications when clinically appropriate
- Occipital nerve blocks with local anesthetic and corticosteroid to reduce pain and confirm diagnosis
- Heat therapy and lifestyle modifications to avoid positions or activities that aggravate symptoms
- For selected patients with refractory pain unresponsive to conservative measures, radiofrequency ablation or other neuromodulation approaches may be considered
Not every patient requires procedural intervention. Treatment recommendations are based on the clinical evaluation, symptom severity, and the individual patient's goals and preferences.
Evaluation
When to Seek Medical Attention.
An evaluation can be helpful if you experience:
- Persistent sharp or shooting pain in the back of the head or scalp
- Pain that affects your quality of life, sleep, or daily functioning
- Scalp tenderness that limits your ability to brush hair or wear certain items
- Pain that has not improved with initial conservative treatment
- New or changing head pain patterns that concern you
- Difficulty distinguishing between occipital neuralgia and other headache types
A clinical evaluation can help determine whether occipital neuralgia is the underlying cause and guide appropriate treatment planning.
FAQ
Frequently Asked Questions.
What is the difference between occipital neuralgia and migraine?
Occipital neuralgia is characterized by sharp, electric, shooting pain that follows the distribution of the occipital nerves (back of the head and scalp), often with a tender point where the nerve emerges. Migraines typically present with throbbing pain, light sensitivity, nausea, and other associated symptoms. Though occipital pain can sometimes accompany migraines, they are distinct conditions requiring different evaluation approaches. A clinical evaluation can help clarify which condition or combination of conditions is present.
What is the greater occipital nerve?
The greater occipital nerve originates from nerve roots in the upper cervical spine and travels upward through the neck muscles to supply sensation to much of the back of the scalp. Irritation or compression of this nerve at various points along its course can produce occipital neuralgia symptoms.
What causes occipital neuralgia?
Occipital neuralgia can result from irritation or compression of the occipital nerves. Causes may include tight muscles at the base of the skull, trauma or whiplash injury, cervical spine pathology, nerve compression from other structures, repetitive neck strain, or poor posture. In some cases, no clear precipitating cause is identified.
How is occipital neuralgia diagnosed?
Diagnosis is primarily clinical, based on the patient's description of symptoms, their location and character, physical examination findings (including palpation for tenderness along the nerve pathway), and reproduction of symptoms with specific maneuvers. Imaging may be considered in some cases. Occipital nerve blocks can be both diagnostic and therapeutic — a positive response to a nerve block can support the diagnosis.
What treatment options may be considered?
Treatment options include physical therapy and neck stretching to address muscular tension, medications such as neuropathic pain agents, and when appropriate, occipital nerve blocks with local anesthetic and corticosteroid. For selected patients with refractory pain, radiofrequency ablation of the occipital nerve or other neuromodulation approaches may be considered. Treatment is individualized based on the clinical picture and patient goals.
What is an occipital nerve block?
An occipital nerve block is an injection of local anesthetic and often a corticosteroid medication around the greater or lesser occipital nerve. The procedure is performed under imaging guidance to increase accuracy. Nerve blocks may reduce pain temporarily and help confirm that the occipital nerve is the source of symptoms. Response varies among patients, and effects are not permanent.
How quickly do symptoms improve after treatment?
Response to treatment varies. Some patients experience relief quickly, while others improve more gradually. Physical therapy and medication management may take weeks to show benefit. Nerve blocks may provide relief within hours to days, but effects are temporary. Long-term management depends on the underlying cause and may require a combination of approaches.
Is occipital neuralgia a serious condition?
Occipital neuralgia is not life-threatening, but it can significantly impact quality of life due to persistent pain and scalp tenderness. The condition itself does not cause permanent nerve damage, but chronic pain can affect sleep, mood, and daily functioning. Appropriate evaluation and management can help reduce pain and improve quality of life.
Limitations
Important Limitations.
Occipital neuralgia diagnosis and treatment is complex. Response to treatment varies among patients, and not all cases are easily resolved. Some patients experience sustained relief with conservative treatment, while others may require procedural intervention. A formal clinical evaluation is required to determine appropriate treatment for any individual patient.
This page is for general informational purposes only and does not constitute medical advice or create a physician-patient relationship.
Dr. Dardashti sees patients in Mission Hills, California, serving patients from the San Fernando Valley, Santa Clarita Valley, and surrounding Los Angeles communities.
Related
Medically Reviewed by Simon Dardashti, MD, MS·Board-Certified, Pain Medicine & Anesthesiology
Last Reviewed: July 2026