Lumbar Spinal Stenosis
Lumbar spinal stenosis means narrowing of the spinal canal in your lower back. This narrowing can put pressure on nerves, causing pain, numbness, or weakness in your legs—particularly when you walk or stand.
Stenosis is very common. If you have it, you're not alone. Many people develop some degree of spinal stenosis over time, particularly as they age. The good news: most people with lumbar stenosis improve with appropriate conservative treatment.
This page explains what stenosis is, how it's diagnosed, why imaging findings don't always predict symptoms, and how different treatment approaches work.
What Is Lumbar Spinal Stenosis?
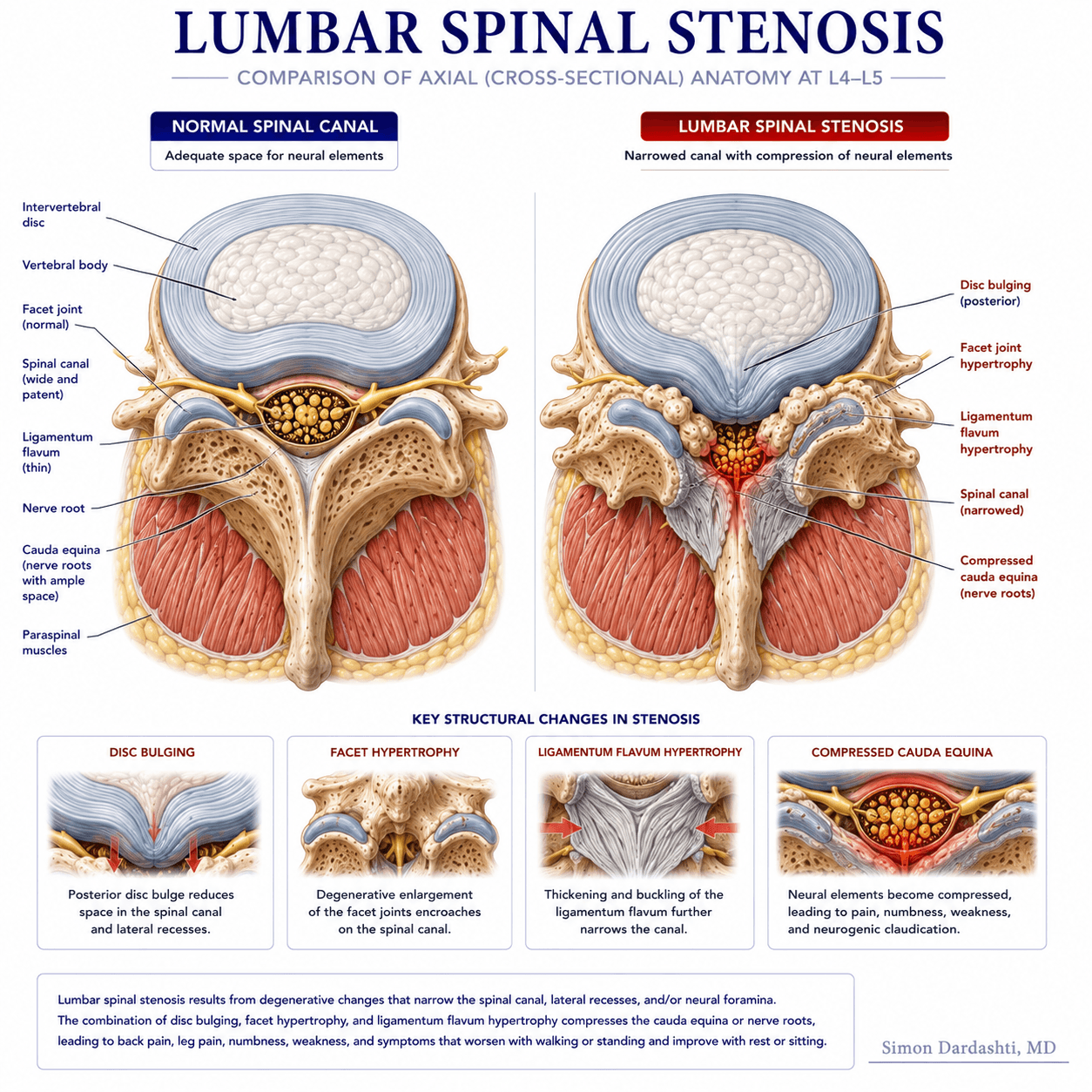
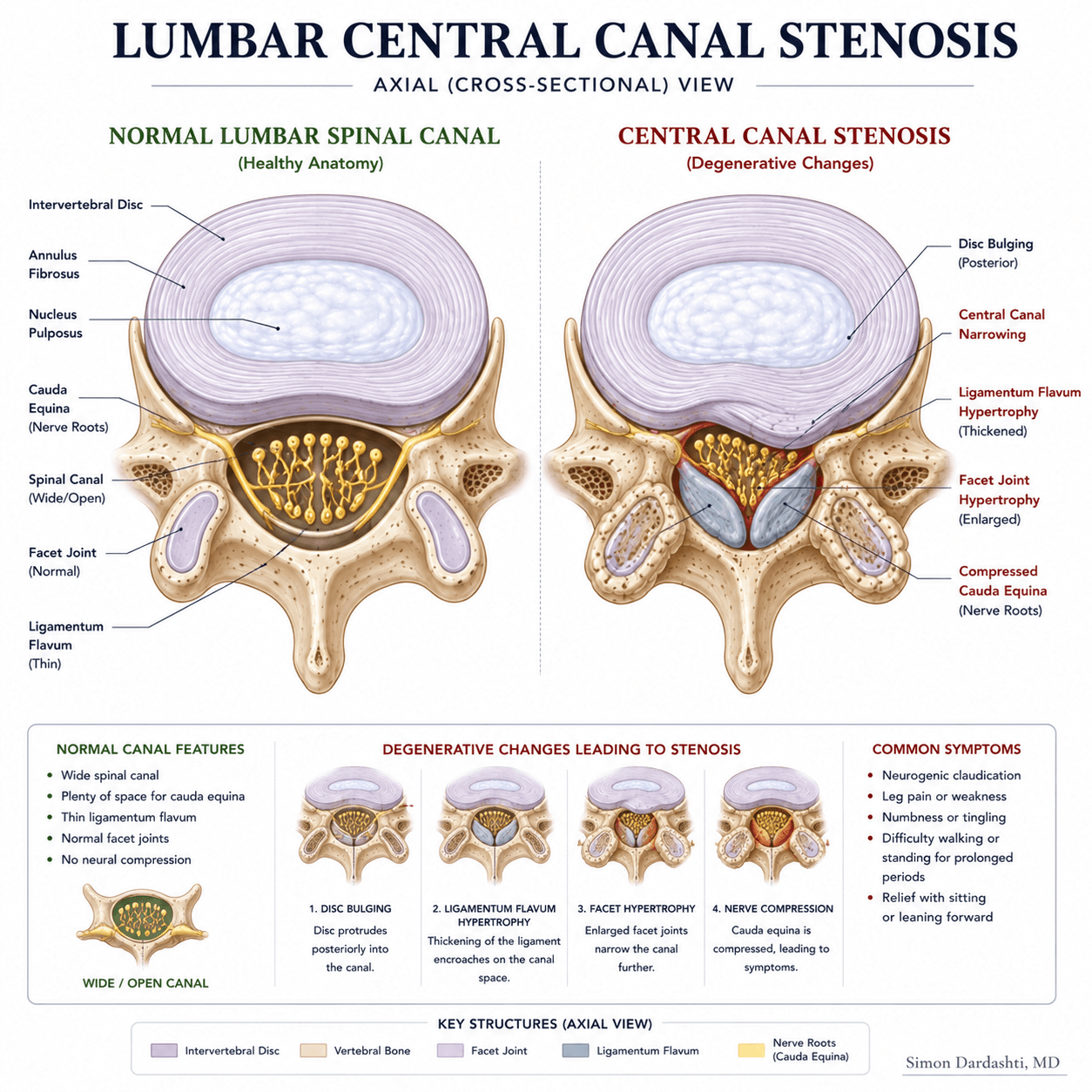
Your spinal canal is the tunnel formed by your vertebrae that contains your spinal cord and nerve roots. In lumbar stenosis, this canal narrows—sometimes from bone spurs, sometimes from disc bulging, sometimes from ligament thickening, or a combination of these.
Stenosis typically develops gradually over years due to:
- Bone spurs (osteophytes): The vertebrae develop extra bone, narrowing the canal
- Disc bulging: Aging discs bulge backward into the spinal canal
- Ligament thickening: The ligaments supporting your spine thicken and reduce space for nerves
- Combination: Most commonly, multiple factors narrow the canal together
Key insight: Stenosis by itself isn't dangerous. It becomes problematic when it pressures your nerves enough to cause symptoms. Many people have stenosis on imaging but no symptoms at all.
Common Symptoms
If stenosis is pressuring your nerve roots, you might experience:
- Leg pain or burning: Usually bilateral (both sides) or more on one side, radiating into the buttocks, thighs, or calves
- Leg numbness or tingling: Often in feet or legs
- Leg weakness: Difficulty lifting foot, feeling unstable, or leg "giving out"
- Claudication: Pain that starts or worsens with walking, improves with rest or bending forward
- Lower back pain: Often present but may be less prominent than leg symptoms
- Balance problems: Difficulty with coordination or stability
Symptoms typically develop gradually and may come and go. Some days are better than others. Many patients notice patterns—walking uphill feels easier than walking on level ground, for example.
Why Symptoms Often Improve When Leaning Forward
One of the most characteristic features of stenosis is relief when you bend forward. This happens because:
When you bend forward (flexion), your spinal canal opens up—the ligaments relax and the canal space increases. This reduces pressure on your nerves, providing relief. Conversely, standing upright or leaning backward (extension) narrows the canal further.
This is why many stenosis patients can:
- Walk easier while pushing a shopping cart (bent forward)
- Tolerate walking uphill better than walking on flat ground
- Feel better walking in a mall where they can lean on railings
- Prefer bicycling to walking (cycling flexes the spine)
Understanding this pattern helps with activity modification—you can structure activities to take advantage of positions that ease symptoms.
Lumbar Stenosis vs Lumbar Radiculopathy
These terms are related but not identical, and understanding the difference helps with treatment decisions:
Lumbar Radiculopathy
Irritation of a specific nerve root, often from:
- Disc herniation pressing on one nerve root
- Nerve root inflammation
- Nerve compression at one specific level
Typical pattern: Pain follows one nerve distribution (L5, S1, etc.). Often sharp, shooting pain down one leg.
Lumbar Stenosis
Narrowing of the central canal affecting multiple nerve roots:
- Usually bilateral or diffuse
- Affects multiple nerve roots simultaneously
- Worsens with certain positions
Typical pattern: Both legs affected (though maybe unequally). Pain worsens with walking/standing, improves with rest or forward bending. More achiness than sharp shooting pain.
Many patients have both—stenosis creating the baseline narrowing with a superimposed disc herniation irritating one nerve root. Understanding which component dominates helps guide treatment.
What MRI Findings Actually Matter
MRI shows exactly where stenosis exists and how severe it is. But here's the important part: imaging severity doesn't reliably predict symptoms or treatment response.
You might have:
- Severe stenosis with no symptoms — You might discover it incidentally on imaging done for other reasons
- Moderate stenosis with severe symptoms — Even though imaging shows moderate narrowing, you're very limited in function
- Mild stenosis with mild symptoms — Matches what you'd expect
What MRI findings DO matter:
- Location correlation: Does the stenosis match where you have symptoms? This suggests it's the cause.
- Severity relative to your limitations: Severe stenosis with severe functional loss may need more aggressive treatment than mild narrowing.
- Emergency findings: Cauda equina compression (rare) or progressive myelopathy requires urgent evaluation.
When Imaging Does Not Match Your Symptoms
Sometimes MRI shows stenosis but it doesn't match your symptoms. For example:
- Stenosis on one side, pain on the other: Your pain likely comes from something else—muscle strain, sacroiliac joint pain, or a different level.
- Severe stenosis but normal exam: If your neurologic exam is completely normal, the stenosis may not be the pain source.
- Stenosis at L4-5 but pain pattern suggests L5-S1: The stenosis at the level shown may not be the culprit.
When imaging doesn't correlate with symptoms, it tells you that the imaging finding may not be causing your pain. This is important because treating the imaging finding might not solve the problem. A careful clinical evaluation helps identify the actual pain source.
Conservative Treatment Options
Most patients with lumbar stenosis improve with conservative care. This typically includes:
Physical Therapy
Specific exercises addressing core stability and movement patterns. Physical therapy often focuses on strengthening while avoiding positions that narrow the canal. Many stenosis patients benefit significantly from structured therapy.
Activity Modification
Structuring your day to favor positions that open the canal (bending forward) and avoid positions that narrow it (standing upright, leaning back). You can often tolerate much more activity if you're strategic about positioning.
Medication Management
Anti-inflammatory medications (NSAIDs) when appropriate, or other medications to manage pain. These often work better for stenosis than for other back pain conditions.
Weight Management
Extra weight increases loading on your spine, worsening stenosis symptoms. Weight loss often provides significant symptom improvement.
Assistive Devices
Canes, walkers, or even corsets can help manage symptoms by providing support or encouraging better positioning.
When Epidural Steroid Injections May Help
Epidural steroid injections deliver anti-inflammatory medication near irritated nerve roots. They may help if:
- Conservative care isn't providing adequate relief. Injections can reduce inflammation and allow you to progress in therapy.
- You want to avoid surgery but are having difficulty with function. Injections may provide enough relief to continue conservative management.
- You need a bridge to more activity. If stenosis limits your ability to exercise, injections might reduce pain enough to increase activity tolerance.
- Stenosis is causing one-sided radicular pain. Injections targeting that specific nerve root may be particularly helpful.
What injections don't do: They don't treat the underlying stenosis (the narrowing is still there). They reduce inflammation, providing temporary pain relief—typically 2-6 weeks, sometimes longer. This gives you a window to benefit from therapy or activity that was previously too painful.
Success rates vary—some patients have significant relief, others minimal benefit. Multiple injections (series of 2-3) are often used to maximize benefit.
When Surgery Should Be Considered
Surgery for stenosis—typically decompression (removing bone spurs and ligament)—should be considered when:
Clear Indications for Surgery
- Significant disability despite adequate conservative care: You've tried 3+ months of appropriate therapy and remain severely limited in function.
- Clear imaging-symptom correlation: Imaging clearly matches your symptoms, and clinical exam confirms nerve involvement at that level.
- Progressive neurologic deficits: You have worsening weakness, numbness, or loss of function despite treatment.
- Severe functional limitation: Stenosis is preventing you from activities that matter to you—work, family time, quality of life.
- Failed conservative management: You've genuinely maximized conservative options and are not improving.
Emergency Surgical Indications
Rarely, stenosis causes cauda equina syndrome—an emergency requiring urgent surgery. This presents with:
- Loss of bowel or bladder control
- Bilateral leg weakness or numbness
- Saddle anesthesia (numbness in buttocks/genitals)
If you develop these symptoms, seek urgent evaluation. But these are rare—most stenosis doesn't become an emergency.
Frequently Asked Questions
How long does it take to see improvement with conservative care?
Most patients notice some improvement within 2-4 weeks of starting structured therapy. Significant functional improvement often takes 6-12 weeks. Some patients see major relief after 3-4 months of consistent effort.
Can stenosis come back after surgery?
Stenosis at the same level can recur over years, but this is less common than many patients fear. Stenosis at different levels can develop. This is another reason to optimize conservative management—it often provides lasting relief without needing surgery.
Should I get a second opinion before surgery?
Yes. Getting a second opinion before spine surgery is always reasonable and recommended. Make sure conservative care has truly been optimized, imaging findings clearly match your symptoms, and you understand realistic surgical outcomes.
Is aquatic therapy helpful for stenosis?
Yes. Water's buoyancy reduces loading on your spine while allowing strengthening exercise—ideal for stenosis. Many patients with stenosis tolerate aquatic therapy much better than land-based exercise initially.
About Dr. Simon Dardashti, MD
Board-Certified in Pain Medicine and Anesthesiology
- • UCLA Pain Medicine fellowship-trained
- • 10+ years evaluating and treating lumbar stenosis
- • Specializes in diagnosis-driven treatment planning
- • Virtual consultations available
Discuss Your Stenosis Diagnosis
If you've been diagnosed with lumbar stenosis and want to discuss your options—whether conservative care is appropriate, whether procedures might help, or whether you need a second opinion on a surgical recommendation—we can help clarify your path forward.
Schedule a Virtual ConsultationVirtual consultations allow us to review your imaging, medical history, and discuss the best approach for your specific situation.
Related Resources
- Pain Without Imaging Findings — Understanding symptoms when imaging seems normal
- Conservative Care vs Injections vs Surgery — Comprehensive treatment pathway
- Second Opinion Before Spine Surgery — What questions to ask
- Lumbar Radiculopathy Evaluation — Understanding radicular pain
- Low Back Pain Evaluation — General back pain assessment
- Epidural Steroid Injections — Understanding this procedure
- Virtual Consultations — Schedule an appointment